A 66-year-old lady presented with epigastric pain, heartburn, regurgitation, belching, high dysphagia and odynophagia. Her OGD showed a hiatus hernia and barium swallows – tertiary contraction and reflux.
Initially high resolution manometry was carried out with a further 24-hour pH-impedance test due to HRM results.
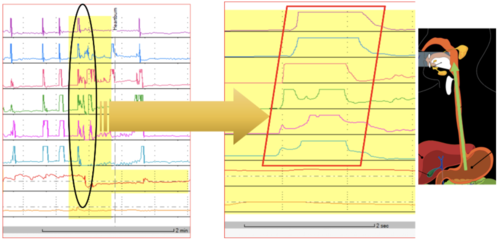
High Resolution Manometry
HRM results showed the following:
- The upper oesophageal sphincter was normotensive and showed complete relaxation on wet swallows.
- The oesophagus produced weak peristalsis with ≥ 50% swallows with DCI , 450U 10/10 weak/failed peristalsis on wet swallows. The patient was reluctant to do solid swallows due to dysphagia, but she did some as she followed the instruction for swallowing solids during the study, which showed a similar profile to water swallows. The patient had difficulty during the rapid water swallows but large volume water swallows showed lower oesophageal sphincter opening.
- The lower oesophageal sphincter was normotensive and showed complete relaxation on wet swallows.
- A borderline sliding hiatus hernia was observed.
These results based on the Chicago Classification showed ineffective oesophageal motility (IOM) with DCI <100 (= failed peristalsis) on 6/10 wet swallows.
A 24-hour pH-impedance study was added due to IOM
24-hour pH-Impedance Reflux Monitoring Off PPI
The pH-impedance reflux monitoring showed the following results:
- Proximal oesophagus: total 5 episodes, normal <31 (impedance).
- Distal oesophagus: total 7.5%, normal < 4.2%; upright 11.3 %, normal <6.3%; supine 3.3%, normal < 1.2%; DeMeester score: 25.7, normal <14.72; number of reflux events (impedance): total 36, normal < 73 (off PPI).
- Reflux symptom correlations: belching 1 episode, SI = 0% SAP = 0%; stomach pain 2 episodes, SI = 50%, SAP = 89%; regurgitation 8 episodes, SI = 38%, SAP = 93%; positive SI ≥ 50%, positive SAP > 95%.
Interpretation and Next Steps
- Pathological acid exposure mainly during the day and postprandial period. This was due to swallows inducing reflux events, very often when the patient ingested liquid the reflux event occurred. This was confirmed with the patient who said this occurred with tap water, lemonade and mint tea. Therefore this high acid exposure can be refluxing a mix of ingested acid liquid and gastric acid.
This phenomenon was clearly detected during HRM on the sequence of ‘swallowing 5 ml water – refluxing – swallowing again to clear. This same sequence was also detected on 23-hour pH-impedance recording during the day on numerous occasions. Understandably it was not detected at night. - Weakly positive reflux symptom association for stomach pain.
- The patient may require lifestyle advice prior to any medical or surgical treatment!