The patient was a 53-year-old lady presenting with a cough, LUQ pain and occasional dysphagia. She had previously undergone high-resolution manometry which showed ‘normal oesophageal motility’ based on Chicago Classification. Her previous 24-hour pH-impedance showed mainly pathological postprandial reflux.
A 24-hour pH-impedance reflux monitoring test on PPIs was carried out. The patient was taking 80 mg Pantoprazole in the morning and 300 mg ranitidine at night along with 10 mg BD Metoclopramide.
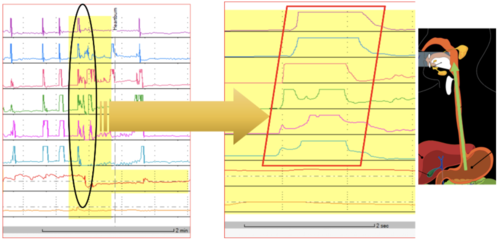
24-hour pH-Impedance Reflux Monitoring
Reflux monitoring showed the following:
- Proximal oesophagus: total 5 episodes, normal <31 (impedance).
- Distal oesophagus: total 0.2%, normal <1.3%; upright 0.4%, normal <1.5%; supine 0%, normal <0.5%; DeMeester score: 1.2, normal <14.72; number of reflux events (impedance): total 45, normal <48 (on PPI).
- Reflux symptom correlations: chest pain 24 episodes, SI = 13%, SAP = 35%; positive SI ≥ 50%, positive SAP > 95%.
- The symptom of LUQ pain was not reported during the test.

Interpretation
- There was no pathological acid or non-acid reflux observed.
- There was no positive reflux symptom association for a cough.
- Gastric pH + 33.0% in total (normal < 55% when on PPIs).
Comment and Next Steps
This was a very interesting case! The reflux study confirmed that PPI medication suppressed acid secretion but it was evident that there was retention of liquid in the proximal oesophagus for extended periods of time in the supine position. This retention can theoretically increase the chance of aspiration and firing the oesophago-tracheal reflex leading to coughing. It was not clear whether this retained liquid was of gastric origin nor was it clear whether the borderline peristaltic large gap in this patient may underlie such pathology. Consideration should be given to the following test-treatment for at least 8 weeks with a follow up review:
- Sleeping in a semi-reclined position.
- Use of alginate products, +/- Azithromycin as a prokinetic agent.
- Investigating for inlet patch (if relevant) as another possible explanation of liquid retention in the proximal oesophagus.
The response to this treatment plan may indeed further confirm the clinical relevance of these findings. The outcome of the above will be of great interest as it may be applicable to help other patients in the future.