A 61-year-old patient presented with chest pain, heartburn, regurgitation and mid/low dysphagia. AN OGD showed mild gastritis and there was no hiatus hernia visible.
High resolution manometry and 24-hour pH/impedance reflux monitoring was carried out.
High Resolution Manometry
HRM results showed the following:
- The upper oesophageal sphincter was hypertensive and showed incomplete relaxation on wet swallows.
- The oesophagus produced panoesophageal pressurisations on ≥ 20% of swallows and no peristaltic contraction.
- The lower oesophageal was normotensive and showed incomplete relaxation on wet swallows.
- There was a 1.3 cm hiatus hernia.
These results based on the Chicago Classification indicated Type II Achalasia (with oesophageal compression). However, there was clear pathological reflux which is not common in achalasia. A small hiatus hernia was also detected by HRM.
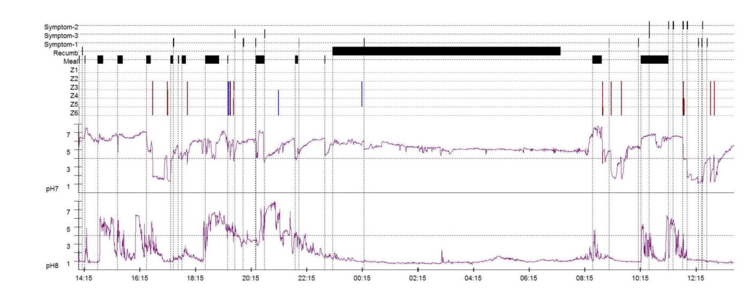
24-hour pH-Impedance Reflux Monitoring Off PPI
The pH-impedance reflux monitoring showed the following results:
- Distal sensor at 31.5 (5 cm above the LSO up-border) and the test showed gastric acid starting from 39 cm (LOS lower-borer) and IP at 40.1 cm (indicating a small hiatus hernia).
- Proximal oesophagus: total 0 episodes, normal <31 (impedance).
- Distal oesophagus: total 12.5%, normal < 4.2%; upright 20.9%, normal <6.3%; supine 0%, normal < 1.2%; DeMeester score: 33.9, normal <14.72; number of reflux events (impedance): total 14, normal < 73 (off PPI).
- Reflux symptom correlations: chest pain 10 episodes, SI = 10%, SAP = 0%; regurgitation 2 episodes, SI = 50%, SAP = 0%; heartburn 5 episodes, SI = 0%, SAP = 0%; positive SI ≥ 50%, positive SAP > 95%.
Interpretation and Next Steps
- Type II achalasia was indicated however since there is clear pathological reflux which is not common in achalasia, pseudo-achalasia resultant from chronic acid reflux (not a common aetiology) or other causes such as malignancies need to be excluded (EUS/CT Scan). A treatment plan could potentially include hiatus hernia repair and gastroesophageal junction dilatation.
- High intra-gastric pressure (>20 normal is about 6 – 10 mm Hg) may influence GORD.
- Post treatment re-evaluation could be valuable for the future approach to this patient as literature is lacking in the area particularly using pH-impedance monitoring.